+977-9856049996

By Susmita Khadka, Project Assistant, Smart Health Global | Field visit report — Bajura and Baitadi Districts, Sudurpaschim Province, Nepal Reading time: 6 minutes | Category: Field Reports
The Walk That Changes Everything
The road into Bajura does not ease you in gently.
It winds upward through terrain that does not forgive mistakes — steep drops on one side, loose stone underfoot, and a sky so clear it makes the distance feel deceptive. From Martadi, the district headquarters, reaching some of the villages we were visiting meant walking for hours on paths that no vehicle could follow.
I am Susma Khadka. I work as a Project Assistant at Smart Health Global, and this was my first field visit to Bajura and Baitadi — two of Nepal’s most remote districts, in the far western Sudurpaschim Province.
I had read the reports. I had seen the data. I thought I understood what “limited healthcare access” looked like on a spreadsheet.
I did not.
What Healthcare Looks Like Before Telehealth
In Bajura and Baitadi, getting sick is expensive — not because medicine costs too much, but because reaching a doctor costs everything.
The people I met in these communities — farmers, mothers, young children, elderly grandparents — told me the same story with different details. A headache becomes a week of worry because the nearest health post is a three-hour walk. A fever that a doctor could diagnose in ten minutes is watched, and waited on, and hoped away, because the alternative means losing a day of work and the money for transport to the district hospital in Dhangadhi or Nepalgunj.
Minor health problems, left untreated long enough, stop being minor.
Before the Smart Health program was introduced, this was simply the reality. Not a policy failure to be fixed at some point in the future — an everyday reality that shaped how people thought about their own health. You did not go to a doctor unless you were serious enough that you had no choice.
The health posts in these communities were staffed by dedicated, trained auxiliary health workers — people who showed up every day and did their best. But they were doing it largely without specialist support, without a reliable patient records system, and without any mechanism for getting clinical guidance when a case was beyond their training.
They were, as one health worker told me quietly during a field observation, “alone with the decision.”
The Moment Things Changed
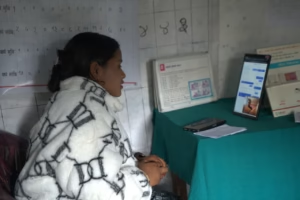
I was sitting in on a telehealth consultation at a health post when I first felt what this program actually means.
A patient had come in with symptoms that the health worker was uncertain about — not a crisis, but a clinical situation that called for a specialist’s eye. Three years ago, the health worker would have referred the patient to the district hospital, knowing that many patients in this community simply do not complete those referrals. The journey is too far, the cost too high, the roads too unpredictable.
Instead, she picked up the tablet, opened the Smart Health Toolkit, and placed a call.
Within minutes, a doctor appeared on the screen. A real conversation happened — questions, examination guidance, a clear recommendation. The patient watched this exchange with an expression I have thought about many times since: a kind of surprised relief, as if something she had quietly given up on had unexpectedly arrived.
She would not have to travel. She had her answer. She would be okay.
What the Health Workers Said
Every health worker I spoke to during this field visit had something specific to say about what had changed — and what they still needed.
They were, without exception, enthusiastic about the program. They had seen its value in real cases with real outcomes. But they were also honest, which I appreciated far more than enthusiasm alone.
They told us that the Smart Health Toolkit needed more features — particularly for specific conditions they were encountering regularly in the field. They asked for refresher training, because the best tool in the world loses value when the user’s confidence fades between sessions. They requested that municipalities establish a regular monitoring and support cycle for the health posts — not occasional check-ins, but structured, ongoing engagement.
They also raised something that had not appeared in any report I had read: the question of incentives. Health workers in these communities carry enormous responsibility and often do so at personal cost. Recognising that dedication — formally, not just informally — matters for sustainability.
I wrote down everything they said. This is what field visits are for.
The Challenges We Cannot Pretend Away
I want to be honest about what we saw that was difficult, because a field report that only tells the good news is not a field report — it is a press release.
Connectivity. In several facilities, the internet connection during telehealth consultations was unreliable enough to cause real disruption. Poor video quality and dropped calls compromise the clinical experience for both the health worker and the patient. This is partly a technical problem we can work on — low-bandwidth optimisation, better compression, offline functionality. But it is also an infrastructure problem that lies beyond any single organisation’s control until Nepal’s telecommunications network reaches these areas more reliably.
Medicines and lab services. A telehealth consultation can produce a diagnosis and a prescription. But if the prescribed medicine is not available at the health post, the patient is back to square one. In several facilities we visited, essential medicines were inconsistently stocked. Health workers were doing their best to source medicines from nearby district hospitals — a workaround that requires dedication and time that should not be required. This is a supply chain challenge that the program alone cannot solve, but one we are actively raising with municipal and district health authorities.
The bright spots. At Kolti Hospital and Pandusain Health Post, the situation was markedly better. Lab services were available. Essential medicines were stocked. The telehealth consultations we observed there ran smoothly, with good connectivity and a health worker team that was confident and well-prepared. These facilities showed us what the program looks like when the surrounding system works. They are the model we are building toward everywhere else.
What Happened When the Community Saw It Work
Change in health-seeking behaviour does not happen because of a policy document or a training session. It happens because of one person watching another person get better.
The community response to telehealth in these villages was initially cautious. Some residents were unfamiliar with the technology. Some were sceptical that a doctor on a screen could know what a doctor in a room could know. A few, frankly, were not sure they were worth the effort of a real consultation.
That last part is the piece that stayed with me longest.
But after watching successful consultations — after seeing their neighbours walk away with diagnoses, with prescriptions, with plans — the community’s confidence in the system grew. Patients began coming to health posts with less hesitation. Health workers reported that the volume of consultations was increasing as word spread.
The most common feedback from community members was something that sounds simple but represents a significant shift: they no longer felt they had to choose between their health and their livelihood.
“I used to have to take a full day off work and pay for a bus to see a doctor,” one patient told our team. “Now I can come here in the morning and be back for my afternoon work.”
What I Brought Back
I came back from Bajura and Baitadi with sore feet, a full notebook, and something harder to name — a clearer sense of what “healthcare access” actually means when you have seen its absence.
The Smart Health program is working. The evidence for this is not in our statistics alone — it is in the faces of health workers who no longer feel alone with the most difficult decisions, and in the patients who arrived uncertain and left with a plan.
But there is real work still ahead. Connectivity, medicine supply, sustained training, municipal monitoring, and health worker recognition are not optional extras — they are the difference between a program that works for a year and a program that transforms a health system for a generation.
The communities of Bajura and Baitadi are not waiting for the world to come to them. They never were. They have been managing, adapting, and surviving in one of the hardest healthcare environments in the country, largely without the tools they needed.
Smart Health Global exists to change that. And visits like this one are how we stay honest about how much further we have to go.
About The Author

Susmita Khadka is a Project Assistant at Smart Health Global, based in Nepal. She supports field implementation, monitoring and evaluation, and community engagement across SHG’s telehealth programs in Bajura and Baitadi districts. This field report reflects her direct observations during a monitoring visit to health facilities in Sudurpaschim Province
If this story moved you, consider supporting our work: [Donate — fund the next telehealth consultation →] Donate